- Mail At drsantanu.surg@gmail.com
- Call For An Appointment (+91) 9830884263
- Online Chatting (+91) 9830884263
Gastrointestinal (GI) cancer surgery offers the chance for a cure to many people. But these procedures are often complex, requiring the skilled hands of experienced gastrointestinal cancer surgeons. Surgery can also be combined with other GI cancer treatments, such as chemotherapy, to improve outcomes.
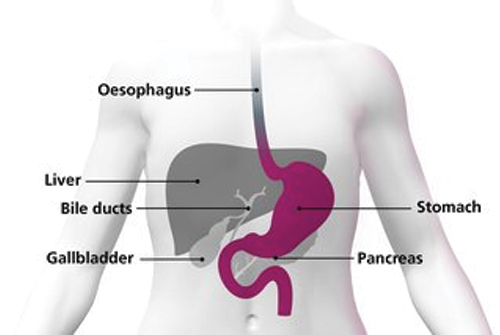
Radical proximal gastrectomy is one of the most commonly used conventional surgeries for gastric carcinoma. Its indications include: small early cancer of the upper stomach; localized cancer in the upper stomach; gastric cancer without metastasis; and gastric cancer with only lymph node station 1 metastasis. A subtotal gastrectomy includes removing the part of your stomach with cancer, nearby lymph nodes, and possibly parts of other organs near the tumor
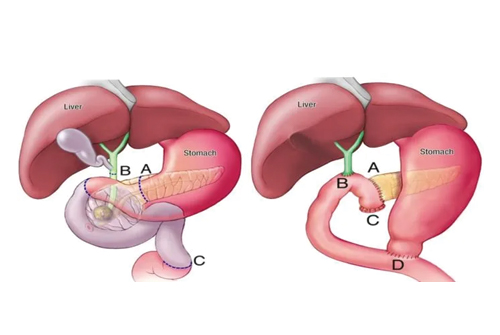
A Whipple procedure — also known as a pancreaticoduodenectomy — is a complex operation to remove the head of the pancreas, the first part of the small intestine (duodenum), the gallbladder and the bile duct. The Whipple procedure is used to treat tumors and other disorders of the pancreas, intestine and bile duct. It is the most often used surgery to treat pancreatic cancer that's confined to the head of the pancreas. After performing the Whipple procedure, your surgeon reconnects the remaining organs to allow you to digest food normally after surgery.
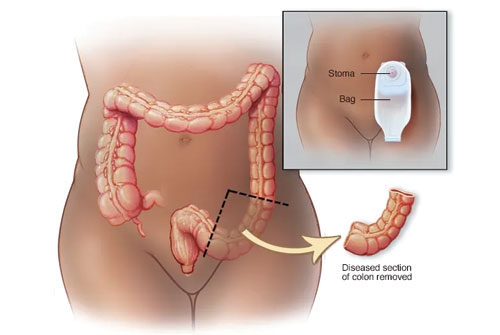
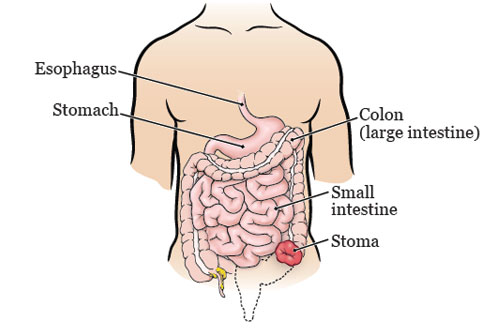
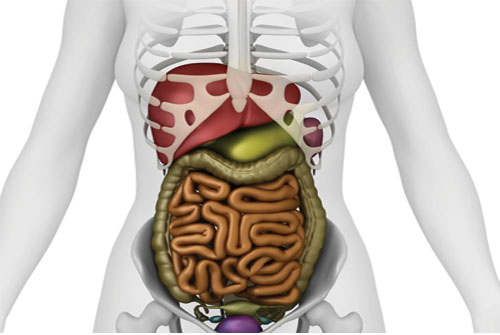
Colectomy is a surgical procedure to remove all or part of your colon. Your colon, part of your large intestine, is a long tubelike organ at the end of your digestive tract. Colectomy may be necessary to treat or prevent diseases and conditions that affect your colon. Colectomy surgery usually requires other procedures to reattach the remaining portions of your digestive system and permit waste to leave your body.
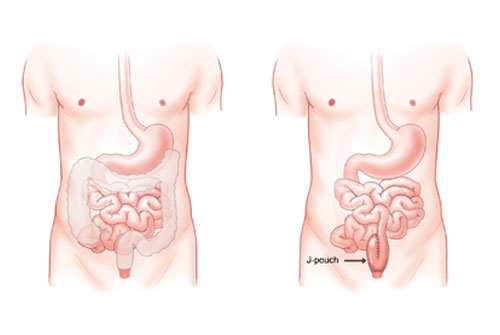
During J-pouch surgery, the surgeon will: Remove the entire colon and rectum, preserving the muscles (sphincter) and opening (anus) at the end of the rectum. Construct a pouch shaped like the letter J from the end of the small intestine and attach it to the anus (opening at the end of the rectum). When possible, surgeons perform J-pouch surgery using minimally invasive (laparoscopic) methods. Instead of opening the abdomen with a relatively large incision (open surgery), they typically make more than one smaller abdominal incision through which surgical instruments and a long, narrow tube with a camera at its tip (laparoscope) can be inserted.
An abdominoperineal resection (APR) is a surgery in which the anus, rectum and sigmoid colon are removed. This procedure is most often used to treat rectal cancers located very low in the rectum. Often this surgery occurs after you have completed radiation and/or chemotherapy treatments. An APR can be done using different techniques. Your surgeon will talk with you about which options are right for you. Depending on what type of surgery you have, your surgeon will make 1 or more incisions (surgical cuts) in your abdomen (belly).
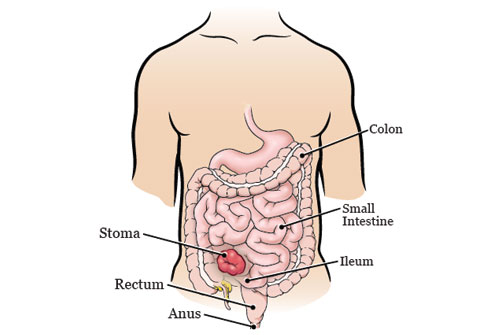
LAR is a surgery that’s done to treat rectal cancer. During LAR surgery, the part of your rectum with the cancer will be removed. The remaining part of your rectum will be reconnected to your colon. You’ll be able to have bowel movements (poop) as usual once you recover from your surgery. LAR surgery can be done using different techniques. Your surgeon will talk with you about which options are right for you. Depending on the type of surgery you have, your surgeon will make 1 or more incisions (surgical cuts) in your abdomen (belly).

Sarcoma is a rare type of cancer that develops from the body’s connective tissues, such as fat, muscle, blood vessels and fibrous tissue. About 20% of sarcomas develop in the back of the abdomen, also known as the retroperitoneum, next to the kidneys. Retroperitoneal sarcomas likely develop over a long period of time undetected and ultimately can grow to massive sizes. It’s not uncommon for a retroperitoneal sarcoma to reach 20-30 pounds. In many cases, symptoms can be vague and nonspecific. The patient may sense a fullness or heaviness in their abdomen. With particularly large tumors, the patient may feel short of breath with exertion or have reflux, constipation or leg swelling. Occasionally, retroperitoneal sarcomas cause pain when they press against a nerve.
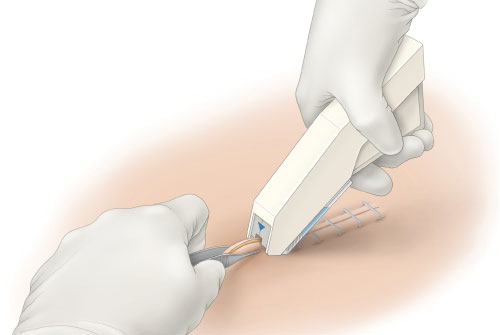
Surgical staplers and staples are medical devices that may be used in place of sutures. They can close large wounds or incisions more quickly and be less painful than stitches for patients. They are often used in minimally invasive surgery. They can also be used to close wounds in areas where skin is tight against bone, in operations to remove organs or to reconnect parts of internal organs. Surgical staplers are generally made of plastic and loaded with a disposable cartridge of surgical staples. The staplers come in both reusable and disposable models. They resemble construction or industrial staplers and are designed to insert and close several staples at once.

When pyogenic liver abscesses develop, it is most commonly following peritonitis due to leakage of intraabdominal bowel contents with subsequent spread to the liver via the portal circulation or in the setting of biliary infection via direct spread. They may also result from arterial hematogenous seeding in the setting of systemic infection. Unlike pyogenic liver abscess, uncomplicated amebic liver abscess generally responds to medical therapy alone; drainage is seldom necessary and is usually best avoided. When drainage is necessary, image-guided percutaneous intervention (ie, needle aspiration or catheter drainage) has replaced surgical intervention as the procedure of choice.
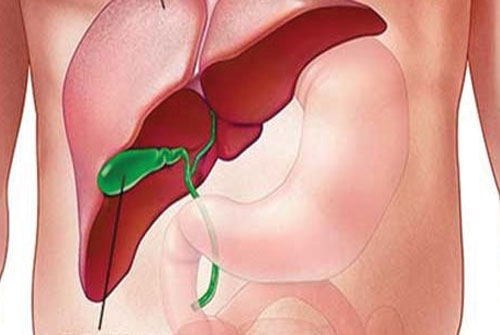
The hydatic cyst occurs by accidental infection of the human with the eggs of Echinococcus granulosus, followed by the development of the larvae, most commonly in the liver (50-70% of cases), and less commonly in the lungs, spleen, kidneys and brain The therapeutic attitude towards hepatic hydatid disease includes the medical treatment, surgical treatment, endoscopic interventional treatment, as well as the subsequent minimally invasive methods.
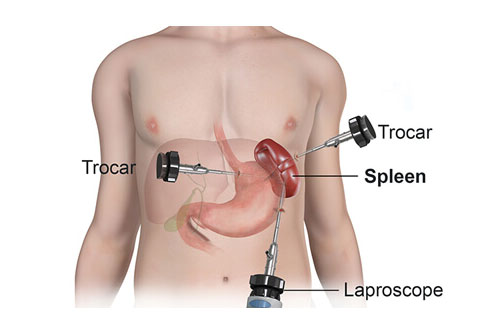
Splenectomy is a surgical procedure to remove your spleen. The spleen is an organ that sits under your rib cage on the upper left side of your abdomen. It helps fight infection and filters unneeded material, such as old or damaged blood cells, from your blood. The most common reason for splenectomy is to treat a ruptured spleen, which is often caused by an abdominal injury. Splenectomy may be used to treat other conditions, including an enlarged spleen that is causing discomfort (splenomegaly), some blood disorders, certain cancers, infection, and noncancerous cysts or tumors. Splenectomy is most commonly performed using a tiny video camera and special surgical tools (laparoscopic splenectomy). With this type of surgery, you may be able to leave the hospital the same day and recover fully in two weeks.
The mainstay of treatment for intestinal perforation is surgery. Surgery for intestinal perforation is contraindicated in the presence of general contraindications to anesthesia and major surgery, such as severe heart failure, respiratory failure, or multiorgan failure. It is also contraindicated if the patient refuses the operation and no evidence of generalized peritonitis exists. Finally, surgery is contraindicated if a contrast meal confirms spontaneous sealing of the perforation (eg, perforated duodenal ulcer) and the patient prefers a nonsurgical approach.
Copyright @2021 Dr. Santanu Sarkar. Designed Kolkata Infotech Solution